How does skull periosteal sinus do?
summary
The most common site of periosteal sinus of skull is at the top of forehead, which connects with superior sagittal sinus through drainage vein, and a few occur in occipital part, which can communicate with transverse sinus. In addition, a few cases have been reported in the skull base. The disease is usually single, and a few patients may be multiple. In the past, according to the causes of periosteal sinus, it was divided into three types: congenital, spontaneous and traumatic. However, due to the slow progress and concealment of the disease, some of the patients with congenital type were found accidentally the day after tomorrow. How does skull periosteal sinus do?
How does skull periosteal sinus do?
Most patients are asymptomatic, some cases are only found by chance, when the tumor increases, local swelling can be felt. Generally, a compressible soft mass can be seen on the scalp, without pulsation. The local scalp can be reddish or cyan blue, and sometimes there are small hemangioma, telangiectasia or vascular nevus on the scalp surface. Any factor that can increase the intracranial pressure can make the mass increase. When standing or sitting, the mass disappears. At this time, the compressed bilateral jugular vein mass reappears. When lying on the back, prone or lowering the head, the tumor increases obviously, and the pores or destruction of the skull can be touched at the lesion.
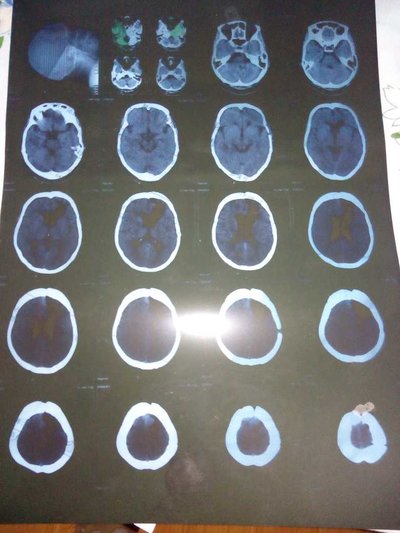
X-ray examination showed that the density of local skull outer plate was slightly lower and several bone foramen of different sizes could be seen in some cases. The venous phase of carotid angiography can sometimes show the lesion, while the whole picture of the lesion and the draining vein can be clearly shown by direct puncture angiography. CT scan showed that the lesions showed slightly high density shadow, and local skull had different degrees of damage and defect. Enhanced scan showed that the lesions showed obvious enhancement effect, similar to the enhancement effect of intracranial venous sinus, but sometimes due to the stenosis of drainage vein or the formation of thrombosis, the enhancement reaction was not big. MRI scan showed mixed signal in the lesion area. Histological examination showed that the lesion was composed of many capillaries and dilated veins without muscle layer.
Intracranial periosteal sinus should be differentiated from cavernous hemangioma, meningocele, dermoid cyst and so on. It can be judged by pressing jugular vein. That is to say, when pressing bilateral jugular vein, the tumor is obviously enlarged, while other types of tumors almost do not show the above signs. X-ray angiography, CT and MRI scanning are helpful for further differential diagnosis. X-ray examination showed that the density of local skull outer plate was slightly lower and several bone foramen of different sizes could be seen in some cases. The venous phase of carotid angiography can sometimes show the lesion, while the whole picture of the lesion and the draining vein can be clearly shown by direct puncture angiography. CT scan showed that the lesions showed slightly high density shadow, and local skull had different degrees of damage and defect. Enhanced scan showed that the lesions showed obvious enhancement effect, similar to the enhancement effect of intracranial venous sinus, but sometimes due to the stenosis of drainage vein or the formation of thrombosis, the enhancement reaction was not big. MRI scan showed mixed signal in the lesion area. Histological examination showed that the lesion was composed of many capillaries and dilated veins without muscle layer.
matters needing attention
Intracranial periosteal sinus should be differentiated from cavernous hemangioma, meningocele, dermoid cyst and so on. It can be judged by pressing jugular vein. That is to say, when pressing bilateral jugular vein, the tumor is obviously enlarged, while other types of tumors almost do not show the above signs. X-ray angiography, CT and MRI scanning are helpful for further differential diagnosis. resection. On the surface of the mass, a sagittal incision across the tumor was made on the scalp to the caput aponeurosis. The cyst should not be cut. Then the cyst was separated passively. After the tumor was completely exposed, the cyst was cut off from the periosteum along the periphery. Sometimes, after cutting off the cyst, it can be seen that the local skull outer plate is smooth and slightly concave, such as funnel-shaped. There is a small hole in the center connecting with the barrier, and there is venous blood outflow. The hole can be sealed with bone wax to stop bleeding. Do not over fill, so as not to cause intracranial venous embolism.